![]()

A smashing success! ISPOR hosted its 20th Annual European Congress in Glasgow, Scotland last month, boasting nearly 5,000 attendees and satisfying our deepest sweet tooth cravings thanks to the lunch menu’s endless supply of teacake biscuits, caramel wafers, caramel shortbread, and IRN Bru. In addition, the conference hosted three well-attended plenary sessions, 28 issue panels, 24 workshops, and more. And we even saw a few rays of sunshine over the weekend!
ISPOR Glasgow Highlight: ICER versus NICE Issues Panel
 One ISPOR Glasgow highlight for me was an issues panel I moderated on Wednesday, November 8th, the last day of the conference. Titled “Should ICER be NICE (or Not)?”, the session had a great turnout – nearly 200 people – and included Dr. Dan Ollendorf, Chief Scientific Officer at the Institute for Clinical and Economic Review (ICER) and Dr. Páll Jónsson, Associate Director at the National Institute for Health and Care Excellence (NICE) as panelists. The goal of the ICER versus NICE session was to compare ICER’s value assessment framework with NICE’s guidelines.
One ISPOR Glasgow highlight for me was an issues panel I moderated on Wednesday, November 8th, the last day of the conference. Titled “Should ICER be NICE (or Not)?”, the session had a great turnout – nearly 200 people – and included Dr. Dan Ollendorf, Chief Scientific Officer at the Institute for Clinical and Economic Review (ICER) and Dr. Páll Jónsson, Associate Director at the National Institute for Health and Care Excellence (NICE) as panelists. The goal of the ICER versus NICE session was to compare ICER’s value assessment framework with NICE’s guidelines.
What’s different between NICE’s guidelines and ICER’s framework?
The differences of ICER versus NICE can be thought of in terms of procedural and technical variations.
Procedural Variations are Minor
For single technology assessments, NICE relies on manufacturers to submit systematic reviews, cost-utility analyses, and budgetary impact analyses while ICER conducts its own analyses. However, for multiple technology assessments, both NICE and ICER conduct their own analyses.
Technical Variations are More Substantial
- Life-extending treatments: NICE allows for quality-adjusted life year (QALY) adjustments for life-extending treatments at the end of life, while ICER does not. More specifically, NICE considers a QALY weighting system that is different from the reference case, in which QALYs in the later stages of terminal diseases are given greater weight (see Section 6.2.9-6.2.12 of NICE’s guide to the methods of technology appraisal 2013).
- Rare diseases: For diseases with a prevalence of two per 100,000 or less, NICE allows for a higher cost-effectiveness (CE) threshold and QALY weighting. In fact, NICE’s CE threshold of £100,000/QALY gained is three to five times higher than the range for non-orphan drugs. Additionally, NICE weights QALYs by a pre-defined factor if the difference in QALYs between the primary intervention and comparator reach certain limits. For instance, if QALYs gained for an intervention relative to a comparator over a lifetime are 30 or higher, those QALYs are weighted by a factor of three. In contrast, ICER increases the CE threshold, but does not allow for QALY weighting. ICER broadens the CE threshold range to $50,000-$500,000/QALY gained (from $50,000-$175,000/QALY gained for non-orphan drugs).
- Budgetary impact analyses: While NICE incorporates a budget impact threshold based on the National Health Service’s budget realities, ICER incorporates a threshold based on the US’s GDP growth and FDA approval volume.
How are NICE’s guidelines and ICER’s framework the same?
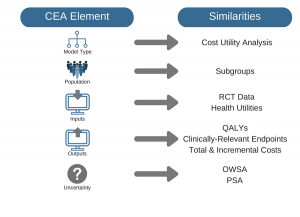
Along with the minor variations above, we also discussed a number of similarities between the organizations:
Overarching Goals
Both organizations use clinical and economic evidence to improve population health and the quality of care and to allow for more efficient use of healthcare resources. They do so through cost-utility analyses, focusing on assessments of the incremental cost per QALY gained.
Disaggregated Results
Both organizations support analysis and reporting of disaggregated results, such as QALYs from different health states, the number and associated costs of clinically-relevant endpoints (e.g., strokes averted among an AF population), as well as total and setting of care costs.
Uncertainty Analysis
Both organizations analyze uncertainty by conducting scenario analyses (i.e., variations in circumstances) along with one-way and probabilistic sensitivity analyses (i.e., variations in inputs).
What was the key takeaway of the ICER versus NICE Issues Panel?
At the end of the day, ICER versus NICE aren't that different. It was agreed that most of the observed differences between the two are at the margin, so the results and interpretations may not vary substantially. Moreover, because the two organizations are working toward the same goal (i.e., to improve population health, quality of care, and efficiency), the organizations could easily morph into one another were they to switch geographic regions. That is, NICE would likely adopt ICER’s US-centric principles if it worked within the US’s regulatory, political, and health system landscape, and vice versa.
ISPOR Posted the Presentation
ISPOR has posted the presentation, which can be found under here under IP20: Should ICER be NICE (Or Not)? How ICER’s New Cost-Effectiveness Framework Compares with NICE’s Guidelines. If you attended the session or if you are reviewing the slides for the first time and have questions, please do not hesitate to contact me.